2021 Collection
FIP’s first ‘Transforming Vaccination’ 2020 programme highlighted the essential role that pharmacists play in immunisation, in addition to the needs and actions required in every region to transform vaccination. What was shared, discussed and Learnt during the programme was published in an FIP collection. The programme culminated in a global Commitment to Action on Improving Vaccination Coverage Through Pharmacies.
What was evident then is that three main concepts emerged in almost every event and every discussion on vaccination: equity, access, and sustainability. All three principles align with three of FIP’s Development Goals: Goal 10 Equity and equality, Goal 18 Access to medicines and services, and Goal 21 Sustainability in pharmacy. It became apparent that vaccination cannot be transformed globally, regionally, or nationally without understanding the implications of equity, access and sustainability on vaccinations – and importantly policy development and implementation.
For that reason, FIP delivered another programme and Commitment in 2021 that shed the light on the different aspects of equity, access and sustainability that are critical in transforming vaccination. This Collection serves the important role of capturing the outcomes of the second programme purposefully and practically, presenting the key insights and outcomes to support our members transform vaccination through policy-based change centered around equity, access and sustainability in pharmacy.
We hope that this Collection, together with all of FIP’s growing resources and programmes of work on vaccination, equity, access and sustainability, all serve to support our members and the pharmacy profession worldwide to truly transform vaccination wherever they are.
Accelerating equity, access and sustainability through policy development and implementation: Summary and highlights
Building on the outcomes of the 2020 programme, the FIP 2021 digital programme focused on supporting FIP members in accelerating equity, access and sustainability of vaccinations through policy development and implementation.
The programme’s twelve digital events were divided into two series. The first of the two series “Towards equity in vaccination globally” comprised five episodes. These included the opening event (which provides much of the work’s context and background described here), alongside four other events which explored equity in vaccinations across the different angles of age, gender, literacy & education, and interprofessional unity & collaboration.
The second of the two series “Sustainability in vaccinations regionally and nationally”
delivered a total of seven digital events. These included six regional roundtables which discussed and identified priorities for sustainable access to vaccinations through pharmacies around the world. The programme's finale event was a global “Leadership Summit on Pharmacy-Based Vaccination Policy and Advocacy” which saw the launch of the FIP Commitment to Action on Accelerating Vaccination Equity, Access and Sustainability Through Pharmacy.
In this programme, we invited experts from around the globe to share their knowledge and expertise around the enablers, barriers, and the important policy changes needed to reduce inequities. Issues around equity in age, gender, and health literacy were addressed, as well as the impact that inter- and intra- professional collaboration. The programme also addressed equity not only among patients and populations, but also among the pharmaceutical workforce itself.
Equity and access are dependent and intertwined; one cannot be reached without the other. Experts discussed strategies and policy changes that can widen access to vaccinations, such as harnessing community pharmacies, investing in vaccination services by all healthcare providers (including pharmacists), and ensuring health system readiness for mass immunisation. Also, widening the access of pharmacists to science information, new therapies, and vaccine manufacturing and delivery services can positively impact vaccination transformation. Access to the workforce is another factor, and so increasing the capacity of the pharmaceutical workforce through education, training, and proper distribution within healthcare systems is key.
Clear strategies to expand vaccination pathways through pharmacies – often the most accessible point in the healthcare system to most people - were proposed to reach people of all ages, gender, or ethnicity in all settings. In countries where there is no health coverage, the cost of vaccinations was also taken into consideration. In those places, not all people can afford a visit to their healthcare provider to get vaccinated, and so pharmacy-based vaccination is considered the more accessible option.
These examples make it important to highlight that policy development is not “one size fits all” issue; policies should address local needs based on its socio-economic factors and the workings of its healthcare system. The need to develop clear policies that ensure all pharmacists are allowed to and qualified to administer vaccines to the population became evident as an accelerator to access. This requires addressing pharmaceutical workforce needs with regards to their development, as well as their participation in the decision-making processes.
Lastly, in terms of sustainability in pharmacy, it is essential that our needs today are met without compromising the needs and resources of future generations. There is a strong emphasis on minimizing the impact of vaccinations on the environment such as the impact that vaccine manufacturing and disposal have. Another important factor addressed is the economic impact that vaccinations can have, especially during emergencies and pandemics. Sustainability is also about ensuring the delivery of sustainable services within the profession, and pharmacy-based vaccination – as the COVID-19 pandemic has shown – is an integral part to both bettering health outcomes and a sustainable profession.
These issues and more were also discussed from a regional point of view during the roundtables. They key insights, lessons and outcomes from the programme’s events are described in more detail in the subsequent sections of this Collection.

The second event of the Transforming Vaccination 2021 programme, “Equity, access & sustainability through life’s ages and stages: Enabling a life course approach to vaccination”, was a live interview with Jane Barratt, the Secretary General of the International Federation on Aging (Canada), along with two bonus interviews that were held offline. Afterwards, and to provide more expert views, two additonal interviews were recorded by FIP. The first was held with Lois Privor-Dumm from the International Vaccine Access Center, Johns Hopkins Bloomberg School of Public Health (USA), and the second interview was with Daphne Holt, the Chair of the Coalition of Life Course Immunisation (UK). This section summarises the outcomes from all three interviews collectively.
Health equity is only achieved when there are no differences in the quality of healthcare provided among all groups and at all ages in a society. Whether to an infant, a child, a young adult, or an older adult, the quality of healthcare should not change. Similarly, the quality of care should not vary throughout an individual’s life. Because inequities are cumulative, their impacts are not confined to one stage of an individual’s life but rather remain and affect a person's life years afterward. In addition, the impacts are not restricted to that individual only, but can affect the lives of those around. Vaccine inequities too, especially among people of different ages, have a cumulative effect. Inequitable access to vaccines not only leaves people at risk of contracting and spreading deadly viruses but also leads to more virus variants emerging, affecting a whole population, even those vaccinated.
The life course approach to health recognizes that health is not shaped by the present moment, but rather by a series of events that occur throughout life. Life course vaccination too is a never-ending process of disease prevention and health promotion that does not stop at a certain age, and is just as important during childhood as it is at older age. It starts with shifting the narrative from focusing on children's vaccines to lifetime vaccines and requires expanding accessibility to and delivery of vaccines from a healthcare setting to a wider community setting. Harnessing the power that pharmacists and community pharmacies have on vaccine promotion and delivery is key for implementing the life course approach to health and to vaccination for several reasons.
First and foremost, the presence of pharmacies in every community, often open 24 hours of every day of the week, allows for the easy, convenient access of community members to a health facility. For that reason, pharmacies can help overcome the barrier of difficult, costly transportation to and from a healthcare facility, especially for receiving vaccination. This is also important for the vulnerable, the immunocompromised members of society, as well as the older adults who have been marginalised during the COVID-19 pandemic, and for whom entering a hospital or a crowded healthcare facility exacerbates their risk of contracting infectious diseases. Bringing vaccines closer to the people can significantly increase vaccine uptake rates and can lower the risk of the spread of a disease. For that reason, vaccination uptake rates have significantly increased in countries where pharmacists can administer vaccines, and have a potential to increase in countries where they do not.
Secondly, pharmacists play a big role in building trust between the healthcare system and a community for the simple reason that the pharmacists themselves are usually part of that community and often see their patients more than any other health provider does. Any member of a community, at any age, can walk into a pharmacy at any time and have his/her inquiries or concerns addressed. Pharmacists can therefore build a bond with members of society better than any other healthcare provider could. Furthermore, different needs and different ways of communication are required at different stages in life. Having a customised communication strategy to every age group is key in health and vaccine promotion. In most countries, information regarding vaccines is usually found online, such as on official websites and on social media. Although access to this information could be very easy for the younger population, it can be very difficult for older adults. Older adults usually need to physically see a health provider who can speak to them in a slow, clear manner using simple language. This is where the convenient access to community pharmacies and pharmacists offers a plain, simple solution to reaching every member of society while addressing vaccine hesitancy and increasing health literacy. Involving pharmacists in vaccination allows them to address the many questions that are asked by anyone and at any time on vaccines, their benefits, and their side effects.
The cost of vaccination, or even the course to reach a health facility to receive a vaccine, can be a burden and a hindrance, particularly for the poorer communities. Paying a visit to a general practitioner to follow up with a vaccine schedule, especially for children who require several visits a year, can be costly. Offering free or affordable vaccines at a close community pharmacy can lift this burden and increase vaccine uptake and adherence.
A few policy changes that can take place today to transform vaccination and close the vaccine inequity gaps at different ages include the standardisation of vaccine schedules for all ages with a centralized system that shows patient records of what vaccines have been received. This allows all healthcare providers, including pharmacists to keep track of what vaccines have already been taken and which ones need to be administered to patients. In addition, national immunisation plans that are comprehensive and fully funded are essential. Adequate financing and strengthening of the supply chain of vaccines is essential to ensure that the vaccines are available for everyone. However, this also highlights the importance of strengthening the demand for vaccines by addressing vaccine hesitancy and health literacy of communities while taking into consideration the communication strategy used with every age group. Setting strong communication strategies that are tailored to match the needs of all age groups helps build trust between health systems and communities, making people feel heard and have their concerns addressed.
To watch all interviews, click here.
In the third event of the first series of the programme, “Vaccinations and the genders: Examining inequities in gender access and handling of vaccinations globally to inform pharmacy policy”, three panellists joined in to share their knowledge and expertise on the gender gaps in vaccine equity. Samiratou Ouedraogo (Canada/Burkina Faso) is Population and Global Health Researcher, Consultant and Advocate at McGill University’s Quebec National Public Health Institute, Member of Women in Global Health Francophone West Africa and Member of the Gavi CSO Board Constituency. Erica Rosser is a Research Associate at the Johns Hopkins Bloomberg School of Public Health (USA), and Sofia Segura (Costa Rica) is a Professor at the University of Costa Rica and College of Pharmacists of Costa Rica. The three highlighted the issues in gender and vaccine equity from the perspectives of the general public and the health workforce, as well as the importance of setting gender-responsive pandemic plans that are inclusive of every member in society. Below is a summary of the discussions and shared experiences.
Gender and sex play a major role in the health of a population. Not only do they have a social and economic impact on an individual, but they also impact health outcomes, health behaviours, and disease susceptibility and progression rates along with many other factors. To have an equitable healthcare system, it must be recognised that there are different intersectional needs for different genders. The health system should therefore be gender-sensitive and tailored to meet the needs of men, women, and gender minorities. The three panellists remind us that gender impacts a whole population as well as the health workforce, and that gender-sensitive pandemic plans are essential for bridging the gaps in health and vaccine equity.
Unfortunately, among populations, gender inequity in health is more evident among women and girls. In most societies, women have lower status and less control in decision-making, leading to a power imbalance. The societal role that women play as informal caregivers, whether as mothers or housewives and having to care for other household members, limits the ease of access to healthcare and vaccines that men can have. In some societies, men have the upper hand and can have complete power within a household, in which some women aren’t allowed to work and hence are financially dependent on men. These women therefore do not have freedom of choice, mobility, or easy access to healthcare and vaccination. Domestic violence has also increased during the pandemic, exacerbating the gender inequity gap further.
Women can also have very limited access to health information due to the reasons mentioned, which leads to higher levels of vaccine hesitancy. During the COVID-19 pandemic, the unclear, shifting regulations on the COVID-19 vaccine for pregnant women and its side effects on fertility and reproductive health have increased vaccine hesitancy among women too. Sadly, some women can even face sexual exploitation in return for receiving healthcare and vaccinations in some countries. Furthermore, the current pandemic has had adverse effects on women and girls due to the limited access to sexual and reproductive health services. This has caused poor family planning, higher risks of unintended pregnancies and sexually transmitted diseases, as well as inadequate healthcare during pregnancy and birth.
This gap in equity can also be observed in the health workforce. Although women comprise 75% of the health workforce, they only occupy up to 25% of the leadership positions. During the COVID-19 pandemic, most frontline workers were women who had to face greater risks of contracting COVID-19 and work extra hours with little or no compensation. Some even had to work with limited personal protective equipment and little training, not to mention having to be part of an unsafe working environment.
For those reasons, it is important to ask who makes the decisions and who suffers the consequences. Having a gender-neutral health system and pandemic plan is not feasible but would rather exacerbate the existing inequities. Strategies and policies must be data driven. Using ethical and safe data collection and analysis – especially data on gender – for developing, implementing, and evaluating gender-responsive pandemic plans is essential. Setting collaborative strategies among policy makers, the healthcare system, including pharmacy and pharmacists, and the community (including informal caregivers) using gender-driven data can help ensure that no one is left behind. Providing healthy, safe work environments where women are given equal opportunities in decision making and leadership as men, and where all voices are heard, including those of women healthcare workers, can also reduce the existing inequities.
To watch the full event, click here.

The fourth event, “Health illiteracy and vaccine misinformation as determinants for equity: developing policies to establish access to quality information in an equitable way”, focused mainly on the strong impact that health and vaccine literacy has on vaccine equity and uptake. The four speakers at the event are Mujahidhussein G Valji, Chief Pharmacist, Aga Khan Health Services (Tanzania); Régis Vaillancourt, Pharmacy Consultant (Canada); Fiona Stanaway, Senior Lecturer in Clinical Epidemiology, University of Sydney School of Public Health (Australia); and Hannelie Meyer, Professor in the School of Pharmacy, Sefako Makgatho Health Sciences University, and Head of the South African Vaccination and Immunisation Centre (South Africa). The article below summarises the event’s key messages.
Before diving into the impacts of health and vaccine literacy, it is first important to define them. Health literacy is the degree of which an individual is able to find, comprehend, and apply basic health information when making health-based decisions. Vaccine literacy also defines how well-informed an individual is on vaccines, and how well he/she applies this knowledge to make the right health decisions. Vaccine hesitancy is the reluctance or delay to get vaccinated, despite the availability and accessibility of vaccines. Better health and vaccine literacy lead to lower vaccine hesitancy and higher vaccine uptake rates. Contrarily, failing to recognise the importance of health and vaccine literacy can lead to higher vaccine hesitancy and lower vaccine uptake rates.
The WHO’s 3 Cs model, which features complacency, confidence, and convenience, is one of the simplest ways to tackle vaccine hesitancy. Confidence is a necessary element that serves to enhance the overall health of a population, and not only vaccine uptake. Distrust in the health system and government can be a major driver of vaccine hesitancy, especially from vulnerable communities, or ones that face social, economic, or cultural exclusion. Hence, building trust between the community and healthcare system and the policy makers as well as trust in the vaccine efficacy and safety can drastically lower vaccine hesitancy. Convenience, too, can enhance vaccine literacy when the time, place, and context in which vaccines are administered are taken into consideration. Bringing the vaccines closer to the people can remove some barriers, such as affordability and transportation, but it must also be done in a manner that matches the cultural background and language of the people in the community. It is also essential to acknowledge that providing convenient information accessibility can be just as important as having close, accessible vaccination sites. False information can spread like wildfire if the right information is not easily accessible. Furthermore, communication strategies must be tailored to match every part of a population, from the older population who mostly require clear, slow, face-to-face communication from their health providers to adolescents who can easily access information through online platforms, and to the displaced or disadvantaged communities who require specially tailored strategies to match their language and cultural backgrounds. This not only makes getting vaccinations easier and more convenient, but also further strengthens the trust and confidence in the healthcare system. Lastly, complacency can exist where there is low perception of the risks of vaccine-preventable diseases and the benefits of vaccines.
Health care providers, pharmacists included, play a critical role in the success of vaccine programmes as their recommendations have a strong influence on vaccine acceptance. As many community pharmacies are the first port of call for individuals exhibiting health seeking behaviours, it is imperative that the pharmacists speak about the vaccines with scientific knowledge. Pharmacists themselves can speak to the efficacy, safety, potential side effects of the vaccine and can in turn educate their patients. Better educated pharmacists are able to convince patients to get vaccinated while less educated pharmacists do poorer in this regard. In addition to the efforts of mass immunisation clinics, primary care, site-specific clinics, mobile teams, pop-up clinics, workplace clinics and public health units, pharmacies have administered and continue to administer COVID-19 vaccines to members of the public. This aids in the wide-spread distribution of the vaccines.
As for the policies that can be put in place to help increase health literacy, creating and funding vaccine campaigns as well as community engagement and communication programmes can have a tremendous effect on vaccine hesitancy. The pharmacy profession can contribute to vaccination agenda by increasing collaboration with health institutions at local, national, and regional levels. Such collaboration could influence regulatory changes to include pharmacies as registered vaccination sites and also provide the required training, licenses, and certifications for pharmacists to provide immunisation services. Improved health and vaccine literacy among pharmacy staff will empower them to confidently promote vaccines, effectively communicate the risks and benefits of vaccination, encourage trust, improve access to vaccines, and increase vaccine uptake. Pharmacists should also employ a motivational interviewing approach to strengthen people’s motivation for vaccination. In addition, establishing clear communication strategies, community mobilizations and outreaches, and incorporating vulnerable groups in the design of technology can have a positive impact. Legislation should be enacted to prohibit the spread of false information. Mandatory cross-cutting components including media and information literacy should be included in all levels of education along with public health education. All these policy changes can impact the health literacy of a population and lower vaccine hesitancy, and eventually leading to better, healthier population.
To watch the full event, click here.

In the last event of the first series, “Working together across systems to transform vaccination policy”, the five experts panellists (listed and described the event flyer below) emphasised the importance of having intra and inter-professional collaboration and the impact it has on achieving equity. Working together, whether with other governments, policy makers, healthcare facilities, health providers, or even with the population, can reduce existing inequities and carve the way to achieving equitable healthcare.
To transform vaccination, collaboration and cooperation among all stakeholders involved is key. This requires the political will to bring everyone together, from policy makers, suppliers, providers, to the receivers of the vaccines, and to put all their skills to use. Working together to ensure that vaccines are accessible not only to the people, but also to all countries, especially low- and middle- income countries is critical in bringing about this transformation. This is especially important when balancing the levels of supply and demand of vaccines.
As one of the panellists mentioned, countries that have achieved high vaccination rates can start sharing their vaccines with other countries in need. In addition, the sharing of data, expertise, research, as well as innovation and technology on vaccine production among health systems and governments can help increase vaccine supply through supporting local vaccine production in some countries. Similarly, working together to send out clear and consistent knowledge and awareness on vaccines can help increase health literacy, decrease vaccine hesitancy, and thereby increase vaccine demand.
Working together with all stakeholders to eliminate barriers to vaccines can have a major impact on vaccination rates and eventually on equity. Inter-collaboration among governments and policy makers can eliminate some barriers such as out of pocket payments for vaccines to make them free or affordable for the people. Another barrier that can be overcome through collaboration among health providers is the need for medical prescriptions to get vaccinated, which in return can accelerate vaccination and lessen the workload of some providers. Similarly, addressing vaccine hesitancy can be made easier when healthcare providers, especially pharmacists, are involved and empowered to take part in vaccination advocacy and education. In addition, some policy barriers hinder countries from utilising the skills of its healthcare workforce, such as restricting vaccination to general practitioners. This can hold countries back from closing the equity gap not only among its population, but also among its workforce.
All this can be done through a few policy changes that can take place today to encourage collaboration among all stakeholders. Sharing of vaccines, vaccine technology, research, and innovation through waiving intellectual property rights on vaccines can boost vaccine manufacturing and development, especially in countries in need. This also includes having a robust funding policies and mechanisms that address all future pandemics, and not only COVID-19, and that make vaccines affordable for all. In addition, having a multidisciplinary approach that utilises the full skillset of its health workforce is essential in achieving equity in a population and in the health workforce. Setting policies in place that legalise and empower pharmacists to take part in vaccination is key as it not only increases accessibility to and uptake of vaccines, but can also impact vaccine hesitancy levels. Having strong policies and strategies in place that allow for the pharmacists to participate in policy-making decisions, in vaccine manufacturing and administering, as well as in vaccine advocacy can bridge the gap in healthcare access and equity as well as that in the health workforce. This includes preparing pharmacists through vaccination education and training programmes that allows them to participate in transforming vaccination at any time.
To watch the full event, click here.

7.1 The Americas
FIP hosted the “Sustainable and equitable access to vaccines: Establishing priorities and setting policies in the Americas region” through two events on September 30 and October 1 of 2021, conducted in English and Spanish respectively. This was done to ensure we reach and engage all members of the Americas region across its two continents. In both events, our panellists discussed what major strengths and challenges emerged with regards to transforming vaccination in the region as well as what lessons were Learnt and what policy changes are required to achieve equity and equitable access to vaccination, especially during the COVID-19 pandemic. Members who participated represented the United States, Uruguay, Costa Rica, and Colombia.
Strengths:
- Pharmacists and pharmacies are more accessible than other healthcare providers because of their presence in every community and at times when other practices are closed.
- Pharmacists have long been ready to immunise in most countries since vaccination training programmes have been integrated as part of their education.
- Pharmacy technicians in the region trained to immunise have increased in number over time.
- An immunisation registry has been implemented in the region that enables health providers to access and record a patient’s vaccination history, including the type of vaccine and the number of doses received. This helps avoid the duplication of vaccinations and enhances communication among all stakeholders involved.
- Pharmacies remained open during the COVID-19 pandemic providing availability to health services that were not available elsewhere.
- In the USA, the “Immunisation Neighbourhoods” programme allows pharmacists to register vaccines in a collaborative system shared with other healthcare professionals.
- In Uruguay, there is in place a universal and free vaccination schedule.
- In Costa Rica, there is a project focusing on immunisation services in vaccination to advance them in their country, including surveys about vaccination, training of pharmacists, and education/awareness campaigns.
Challenges:
- Weak health infrastructure in some countries making them dependent on other regions/countries for support. This includes a lack of manufacturing facilities and workforce and other resource shortages.
- The spread of vaccine misinformation, particularly ones that play on emotion, has a big effect of the willingness of the people to get vaccinated.
- In the US, each state has its own regulations, causing great differences among states in what pharmacists are authorised to do, including vaccination of different age groups.
- Vaccine storage and handling as well as medicine shortages have proved to be challenging during the COVID-19 pandemic.
- Rules and recommendations are constantly changing, leading to more confusion.
- In Uruguay, there is a lack of training in the area of vaccination in undergraduate levels
- High heterogeneity in the region in terms of demographics, health systems and policy making, complicating best practice sharing.
- Especially in Venezuela, Jamaica and Haiti, data from 2019 suggests a lower coverage rate of different vaccines compared to the average for the region.
- In Costa Rica and Latin America in general, there was a struggle with vaccine development and production.
Lessons Learnt:
- Strategies around immunisation should include outbreak response, monitoring and surveillance, as well as treatment, and not only vaccination allocation and distribution.
- Empowering pharmacists to advocate and administer vaccines, especially in vulnerable and underserved communities, could be one of the most impactful ways to gain the confidence and trust of a population. Sharing of success stories and not only facts about the positive effects of vaccines increases confidence and trust in the health system and drives a positive behavioural change of the communities towards vaccines.
- Disease surveillance is key in optimising immunisation programmes. Making sure a surveillance system is responsive, comprehensive, and efficient helps monitor disease control and eradication as well as outbreak response.
- Providing free and accessible education resources and recommendations to communities, other countries and even other regions can help battle the spread of misinformation.
- Getting training in countries where the role of pharmacists as vaccinators is already established can help support the development of policies and strengthen this role where it is still not a reality.
Policy Changes:
- Having consistent policies and regulations across the whole region that involve pharmacists in immunisation are critical in achieving equity and equitable access to vaccination.
- Making immunisation programmes a part of primary health care, with effective coordination, financial management, and monitoring and evaluation.
- Strengthening the supply chain to ensure the availability of vaccines everywhere along with coordination and collaboration with other supply chains to ensure effective delivery.
- Proper handling of vaccine waste, from production to disposal, to reduce the environmental footprint that it could have.
- In Uruguay, the national vaccination plan adapted to the emergency vaccination plan and increased healthcare professionals to vaccinate (without the option for pharmacists to vaccinate) - missed opportunity for pharmacy as the legislations did not unlock this possibility.
- The immunisation plan for the Americas region 2015-2020 was the basis of the efforts the region had in vaccination. Currently, the region follows the global Immunisation Agenda 2030.
To watch the full events, click here.


7.2 The Eastern Mediterranean Region
Focusing on the second of six regions, FIP hosted the digital event, “Sustainable and equitable access to vaccines: Establishing priorities and setting policies in the Eastern Mediterranean region”, on 7th October 2021. Expert panellists from Pakistan, Jordan, Bahrain, Lebanon and Yemen came together to give a true regional perspective on vaccines access and equity. Common themes were identified and shared, as well as valuable insights gained from individual country examples in order to build a greater understanding of regional issues, particularly within the context of the COVID-19 pandemic.
Strengths:
- National child vaccination programmes administering free vaccines has reduced mortality rates in children under 5, many of which are due to vaccine-preventable diseases.
- Vaccine mandates in certain professions, such as healthcare.
- A wide range of COVID-19 vaccines being implemented (as seen in Pakistan, which administered eight different vaccines), while ensuring administration is free of charge and widely available, combined with community outreach initiatives to maximise vaccine adoption.
- IT databases and resource management systems to monitor COVID data and enable decision making based on needs assessment, as well as software monitoring levels locally to help avoid healthcare institutions becoming overwhelmed.
- Distribution of accurate vaccine efficacy and safety data and information to encourage adoption among the general population via media campaigns and other methods.
- Encouragement of vaccine manufacture and research.
- Empowering pharmacists as key in the vaccination effort through training and by acting as educators and advisors to facilitate and participate in routine immunisation initiatives – these competencies are being highlighted during pharmacy training.
- Implementation of a national initiative for the administration of emergency vaccines (as seen in Bahrain) which allows rapid and efficient rollout of vaccines in mass outbreak scenarios such as COVID-19.
Challenges:
- So-called “anti-vax” sentiment and false information spread, as well as concerns regarding vaccine side-effects and general vaccine hesitancy.
- Lack of vaccine awareness among marginalised communities.
- Low COVID screening rates leading to underreporting of confirmed cases.
- Cost of obtaining and distributing vaccines, especially for low to middle income countries, as well as barriers to local production capacity due to IP rights and limited technology transfer.
- Community pharmacists not being utilised in vaccination programmes for maximum coverage.
- Lack of mobile clinics and other initiatives allowing the vaccine to reach more rural and isolated communities, as well as the refugee population.
- Countries such as Yemen are also dealing with regional conflicts, partition and rule under separate governments, making a cohesive vaccine initiative and vaccine distribution much more difficult.
Policy Changes:
- Adaptation of a behavioural science approach at a government level which “nudges” the population to get vaccinated.
- Involving key stakeholders such as NGOs, healthcare professionals, and community and religious leaders to enable the spread of vaccine awareness.
- New legislations and training/accreditation to enable pharmacists to administer routine vaccines such as for influenza as well as emergency vaccines (this has been successfully implemented in Jordan).
- Increase authorised vaccination centres to include hospital and community pharmacies.
- Vaccination competency certification and pharmacy registration with the relevant national government bodies.
- Prioritise the review and authorisation of vaccines over other medicines.
- Involve other healthcare experts and qualified professionals in the review process to expedite the approval of vaccines.
You can watch the Eastern Mediterranean regional event here.
7.3 The European Region
Taking place on 14th October 2021, the third in the FIP series, “Sustainable and equitable access to vaccines: Establishing priorities and setting policies in the European region” focused on the regional needs and drivers for transforming vaccination in Europe. Pharmacy experts from Belgium, Poland, the UK and Malta discussed and identified priorities for sustainable access to vaccinations through pharmacies and compared their experiences of the COVID-19 pandemic as well as regional approaches to vaccination.
Strengths:
- Community pharmacies taking on the role of patient sensibilisation to build trust and improve vaccine adoption.
- Pharmacists widely trained in vaccination, both within the pharmacy and in vaccination centres.
- Centralised vaccine distribution with full-service healthcare distributors acting as distribution hubs, as seen with the COVID-19 and flu vaccines in several European regions.
- In countries where pharmacists directly administer vaccines, such as the UK, pharmacies are able to sub-contract pharmacists, support staff and other resources to the primary care network and other primary care GP vaccination sites, as well as hosting vaccination clinics at the pharmacy.
- Regional online CPD programmes targeting pharmacists, pharmacy students and graduates focusing on key competencies.
Challenges:
- Possible legal implications associated with being a pharmacist-vaccinator.
- Shortage of trained vaccinators.
- Dual distribution of COVID-19 and influenza vaccines requires storage capacity, efficient planning and transparency from vaccine manufacturers.
- Political, legal and organisational barriers often prevent pharmacists’ participation in vaccination programmes.
- Lack of financial incentives for pharmacists to provide vaccination service.
Lessons Learnt:
- Clear communication and guidance to healthcare providers on the management of COVID-19 and flu vaccines in tandem is needed.
- Pharmacies should be maximised as a key resource for accessible and convenient administration of both COVID-19 and flu vaccines.
- Studies show pharmacist-led initiatives help improve vaccination rates and access.
Policy Changes:
- Pharmacists expanding their roles into prescription to shorten the patient journey, as evidenced in Belgium where pharmacists can now prescribe and administer the flu vaccine.
- Pharmacists should take the lead in vaccine preparation to increase coverage.
- Use study and research data to strengthen the case for pharmacists as vaccinators.
- Collaboration with key stakeholders including full-service healthcare distributors and pharmacies to ensure vaccine uptake.
- Regional policies should expand to allow pharmacists to train to become qualified in vaccination administration.
- Remuneration models should promote the suitability of pharmacy premises for vaccination.
- Providing a legal basis for financing of pharmacies to deliver vaccines, as shown in the changes to Poland’s Act of Pharmacists Profession, Act of Infectious Disease Prevention and Pharmaceutical Law to enable this.
- Training and accreditation provided, as seen by the Malta Chamber’s implementation of a professional, structured training programme, putting pharmacists in a position to safely give a holistic pharmaceutical care service with full communicable disease management, not just vaccination.
- Creation of coalitions between pharmacists, other healthcare experts and partners to report together on infectious disease and build a consensus of medical, pharmaceutical and nursing environments (as seen in the creation of Poland’s PBI Coalition).
You can watch the European regional event here.

7.4 The South East Asian Region
In the fourth event of the second series, “Sustainable and equitable access to vaccines: Establishing priorities and setting policies in the South East Asian region”, experts from Sri Lanka, India, Indonesia and Nepal joined to share their knowledge on the strengths, priorities, challenges, and policy changes needed to transform vaccination in the Southeast Asian Region. The speakers also shared stories about the COVID-19 pandemic impact in their countries.
Strengths:
- Inclusion in the law: This is observed, for example, in Nepal, where there is an established immunisation act to regulate the equity access for vaccination across populations.
- Some countries in the Southeast Asian region have local vaccine production. For example, Indonesia and India both initiated local vaccine production, and India has exported vaccines for the COVAX project to about 95 countries.
- Success of national immunisation programmes: National immunisation programmes can lead to high immunisation coverage rates. For example, in Sri Lanka, the success comes from the importance of having free healthcare services and vaccines free for all. So, there will be no financial barriers to vaccines. Sri Lanka also has a strong primary health care system, focusing on community engagement and empowerment of the community.
- The use of technology in vaccine distribution: India mentioned the use of drones to transport vaccines to inaccessible areas in India – that is another success story.
- The rapid responses, collaboration, and coordination: This is observed during the COVID-19 pandemic in Sri Lanka, India and Indonesia, highlighting the importance of the coordination across governments, and also across sectors.
Challenges:
- The geographical and demographic challenge: The Southeast Asia region is unique because it is home for over a quarter of the world's population. This is very important because this highlights the challenge in access to vaccines, particularly related to equitable access across the population - across priority groups, such as people with comorbidities, and also across high and low-income communities. In addition to that, there are also challenges to reach vaccination centres, because of the complicated geographical situation.
- The capacity in vaccine production: This is particularly obvious in countries with a lack of funding. Although there are some countries that can produce the vaccine by themselves, there are other countries with lack of funding and don't have capacity for the vaccine production.
- The limited infrastructure: This has been mentioned in other regions. An example from the Southeast Asia region is inadequate refrigeration for vaccine storage. Also, the lack of laboratory testing facilities may affect the equity in vaccination.
- Limited human resources: Pharmacists have no direct role in vaccine administration. Pharmacists can be involved as vaccinators, but they can also be involved in adverse events monitoring, which also has been mentioned previously as well in other regions.
- Public acceptance to vaccines: The resistance and spread of misinformation across the population is one of the challenges that the region faces. This is also observed in other regions. An example is the importance of the clarity for the need of the COVID-19 booster dose.
- The improvement of health information systems.
Lessons Learnt:
- Competency development plays a critical role. An example is integrating public health in pharmacy education to support pharmacists’ role in health emergency. Also, developing their skill set related to vaccination administration can play a vital role.
- Expansion of Pharmacy Workforce Role as Vaccinators is essential. It is also important to advocate and recognize pharmacists as vaccinators to support with the equity and access to vaccination.
- Data Intelligence and Sharing Knowledge can have a tremendous effect. Data and knowledge sharing across countries, also mentioned in other regions, is very important. It can speed up the vaccine transformation across our region.
- Collaboration and Coordination can help bridge the equity gap. Strengthening the collaboration and coordination across sectors and across institutions within the countries and absolutely across countries can play a vital role.
Policy Changes:
- Robust funding mechanism that allows for the local production, proper storage, and equitable distribution of vaccines.
- Authorising pharmacists to take part in vaccination production, administration, and advocacy
- Including vaccination education and training as part of the pharmacy education programmes ensures that all pharmacists will be ready to immunise at all times
- Having campaigns that address vaccine hesitancy and the spread of misinformation
You can watch the South East Asian regional event here.
7.5 The Western Pacific Region
On October 28, 2021, FIP hosted the event “Sustainable and equitable access to vaccines: Establishing priorities and setting policies in the Western Pacific region.” During the event, experts from Singapore, Malaysia, Australia, Philippines shared their knowledge and expertise on the strengths, priorities, challenges, and policy changes required to transform vaccination in their countries, especially in the past 2 years during the COVID-19 pandemic. Although the Western Pacific is a diverse region, with great differences among its countries, some common outcomes have emerged along with a few country examples and success stories that have been shared by our experts.
Strengths:
- Vaccination is part of pharmacy education in most parts of the region along with vaccination training programmes and certifications
- Some countries have a legal framework authorizing pharmacists to take part in vaccination logistics, advocacy, and administration
- The COVID-19 pandemic has revealed the short time span during which come countries built the infrastructure and mobilized the resources required for emergency response. It has also highlighted the importance of a using an interprofessional, multidisciplinary approach and the inclusion of pharmacists in vaccination.
Challenges:
- Funding
Funding was pointed out as a challenge in 2 ways:
-
- Funding of vaccines and making them free/affordable to the public
- Funding pharmacists to take part in vaccination coverage. In some countries, pharmacists are not paid enough or as much as other healthcare professionals to administer vaccines.
- In some countries, pharmacists are authorized to administer certain vaccines to certain age groups and in certain locations.
- Some countries such as Singapore have legislative barriers to vaccinations, such as prescriptions for vaccines.
- The lack of centralized and computerized patient records.
- Lack of availability and awareness on the importance of life course vaccination – not only children vaccination
- Lack of local vaccine production and reliance on overseas supply.
- Lack of evidence shared on the value and role of pharmacists in vaccination
Lessons Learnt:
- To achieve equitable access to vaccination, pharmacy and pharmacists must be more involved in addressing vaccine hesitancy and administration because of their presence and direct contact with almost every community
- Starting small, in one state or jurisdiction, using one vaccine and one age group, can be the best way to start utilizing pharmacy, the profession, and pharmacists in immunisation as it allows for early identification of a country’s capabilities as well as the strengths and challenges that may emerge during the process. Australia has proven that this is a very successful approach since they have started using this strategy in 2014 with the Influenza vaccine
- Interprofessional collaboration is an essential part as it allows for pharmacists to work not only with other pharmacists or pharmacy associations, but also with other healthcare professionals, especially during adverse events in which ‘all hands-on deck’ are needed. In addition, sharing patient records on a national registry plays a critical role in improving health services and allows for data collection for research, monitoring and evaluation. Australia and the Philippines have succeeded in this area as they both have national registries that provide patient information to healthcare providers
Policy Changes:
- Authorising pharmacists to take part in all vaccination-related matters, from advocacy to administration
- Gathering data to show the real value of pharmacists in vaccinations and to monitor and evaluate the services they provide
- Addressing the age gap in vaccination schedules, and paying special attention to adult vaccination schedules, not only children
- Addressing the issue of funding both vaccines and pharmacists to move towards equitable access and therefore equity in vaccination
You can watch the Western Pacific regional event here.

7.6 The African Region
On 4th November 2021, FIP examined the last of the six regions during the event, “Sustainable and equitable access to vaccines: Establishing priorities and setting policies in the African region”. This digital programme focuses on supporting FIP members in accelerating equity, access, and sustainability of vaccinations through policy development and implementation regionally. Speakers from Kenya, Nigeria, Algeria and South Africa gave their expert view on the challenges faced and the successes achieved from a pan-African perspective.
Strengths:
- Partnerships with health authorities and endorsements and support from large organisations such as WHO and FIP to increase vaccine availability.
- Improvements in training and health facility readiness, especially during the COVID-19 pandemic.
- Creating effective narratives around efficacy and safety to encourage vaccine take up among the public and using public role models to convey messages.
- Involvement of the private sector in vaccinating their staff and administering vaccines alongside government programmes – for instance, the Kenya Private Sector Alliance (KEPSA) has successfully vaccinated 70,000 people so far by using its members to fund vaccines and pledge to vaccinate their staff and surrounding community.
- Collaborative training initiatives such as the Pharmacy-Based Vaccination Delivery Training Programme in Nigeria, in partnership with Mercer University, resulting in 161 trained and certified Nigerian pharmacists.
Challenges:
- Availability of finances to enable vaccination training and distribution, and adequate vaccine storage (plus many African countries rely on donors to finance vaccine programmes with less than 50% of funding coming from local and regional governments).
- Reluctance among pharmacists to train to administer vaccines associated with difficulties in acquiring new skills, added responsibility of immunisation, and misunderstanding of legal provisions.
- Difficult to obtain support from politicians and key stakeholders.
- Few if any local vaccine manufacturing facilities and logistical issues in many countries.
- False vaccine narratives leading to vaccine hesitancy in some areas.
- Inequitable distribution of vaccines across regions.
- Community pharmacies not permitted to be used as vaccination centres for COVID-19 in some countries (Kenya, for example) and where vaccination schemes are in place, very few community pharmacies are enrolled.
- Vaccination coverage across many African countries is low – less than 10% of the African population have received a COVID-19 vaccine and 20% of African children have not received all necessary vaccines for full immunisation.
- Initial difficulty in collaboration between private and public sector healthcare providers, with limited access to vaccine appointments after hours.
Lessons Learnt:
- Education is key to enable pharmacists.
- Pharmacists must be more involved in primary healthcare, specifically vaccine administration and advice.
Policy Changes:
- Increased advocacy required to raise the profile of pharmacists in vaccination programmes, plus introduce regulations for them to administer vaccines, as well as establishing trust with other healthcare professionals and encouraging and supporting pharmacists.
- Vaccination training should be integrated into the pre graduate pharmacy curriculum.
- Allowing community pharmacies to be COVID-19 vaccination centres will decrease demand on hospitals and health centres, and will increase coverage.
- For every vaccine made for developed countries, one should be made available for low-to-middle-income (LMIC) countries to encourage vaccine equity.
- Integration of vaccination initiatives into routine services (outreach programmes, community vaccination schemes etc).
You can watch the African regional event here.

In the programme finale, “The Leadership Summit on Pharmacy-Based Vaccination Policy and Advocacy”, which was a high-level event in which global leaders from health and pharmacy joined to recap the primary outcomes of the 12-event digital series and to launch the FIP Commitment to Action on Sustainable and Equitable Access to Vaccines Through Pharmacy. This FIP Commitment is based on the outcomes of the 2021 transformation programme and will carve the pathway for integrating pharmacy-based vaccination within life-course immunisation. The Commitment and its ten statements are shared below.
FIP commits to transforming vaccination by accelerating vaccine equity, access and sustainability through:
Global and regional applicability:
- Supporting countries with accelerating policy development, implementation and transformation, through advocacy, guidelines and support.
- Identifying the needs, priorities and challenges of every region through needs-based policy development.
Life-course immunisation:
- Recognising the impact of pharmacy-based vaccination delivery on disease prevention throughout life’s ages and stages from childhood (including pregnancy) to late adulthood.
- Supporting countries to develop policies that enable pharmacies and pharmacists to deliver integrated vaccination services throughout the life-course and as part of wider national immunisation policies.
Gender:
- Recognising the multi-faceted impact of gender on vaccination access, delivery and policy, and the inequities in gender access to vaccines to inform pharmacy policy.
- Supporting countries to develop policies that accelerate equitable access of vaccinations to all genders, empower women as caregivers to support vaccinations, mitigate the impact of COVID-19 on gender inequity, and address the issues around gender inequity in the workforce (which is especially important to discuss in 2021 Year of the Health Worker).
Health literacy:
- Recognising the impact of health literacy and vaccine hesitancy on vaccine uptake and sustainable access, disease prevention, and the overall health of the population and integrating it in policy setting.
- Supporting countries to develop policies that empower pharmacists to address health literacy and reduce vaccine hesitancy, misinformation and disinformation in all parts of society by building trust through effective communication and easy access of correct and accurate information to patients and the public.
Working together:
- Recognising and fully harnessing the power of interprofessional collaboration as a driver to achieving equity, accessibility and sustainability in vaccination.
- Supporting countries to develop policies that allow for the sharing of data and technology around vaccination as well as utilising a multidisciplinary workforce to make vaccinations equitable, accessible and sustainable.
Following the Summit, a closed invitation-only Leadership Roundtable took place. Key FIP leaders joined from Bureau, the regional Forums, Boards, FIPEd and Young Pharmacists Group (YPG) to discuss the implementation of the 2021 Commitment. This section captures the key outcomes of the roundtable.
FIP’s “Transforming Vaccination” agenda is aimed at increasing global vaccination coverage by addressing the important role pharmacists play in saving millions of lives through the provision of vaccination services. Hence, FIP commits to expanding vaccination pathways through pharmacies and pharmacists, expanding the pharmacist’s scope of practice and education to include vaccination administration, investing in prevention strategies to foster equity and sustainability in vaccination delivery. The concepts of equity, access to medicines and services, and sustainability in pharmacy are non-negotiable in the vaccination transformation agenda. To accelerate global vaccine equity, access, and sustainability, FIP considers integrating pharmacy- based vaccination into life-course immunisation (vaccination delivery throughout life’s ages from childhood to adulthood). Several factors are considered to inform the development of an action plan to drive the life-course immunisation goal.
Parts of the Commitment that FIP should prioritize implementing in the coming 1 - 3 years
All areas of the commitment are important but participants recommended focusing on policy development and advocacy over the next 1-3 years. At all levels (globally, nationally, regionally), there should be policies that favour the inclusion of pharmacists in immunisation programs. The COVID-19 pandemic highlighted the importance of pharmacists in pandemic response and particularly, and their role in improving vaccination coverage. This momentum can be maintained and utilized as a basis for the involvement of pharmacists in immunisation services. Global and regional applicability can be evaluated based on country/regional needs to identify effective ways of developing working relationships with several stakeholders in the various regions. Guidelines and frameworks from countries where pharmacists offer vaccination services could be collated and arranged to form a database. This would provide easily accessible materials for pharmacy organisations in countries that do not allow pharmacy-based vaccination services to study and adopt these frameworks to their local and regional needs to support their immunisation advocacy efforts
Life-course immunisation will be non-existent if vaccines are unavailable. Vaccine shortages will truncate all efforts to increase coverage and hamper pharmacy-based vaccination service delivery. Thus, deliberations on establishing a globally reliable and equitable vaccine supply chain system with pharmacists integrated into the system will be pivotal in achieving whole life-course immunisation. Pharmacists’ knowledge, skill, and competency in vaccination services should be boosted by incorporating vaccination courses in undergraduate and continuous professional development programs. Technology could be used to facilitate this process by developing certified self-paced courses on vaccination.
Considerations to be made by FIP when implementing the Commitment
Pharmacists as vaccinators is a natural progression of the pharmacists’ role and is aimed at improving global vaccination services. Because pharmacy-based vaccination services are not supported in many parts of the world, emphasis should be placed on downplaying competition but rather promoting collaboration, cooperation, and respect with other professional organizations. This will help develop an environment that portrays pharmacists as contributors and not competitors. Ties with relevant stakeholders and organizations including the WHO, UN, etc. can be strengthened by inviting key players to pharmacy events to discuss vaccination.
Hurdles should be anticipated and potential solutions prepared to mitigate them. A roadmap could be developed to highlight and address the needs and barriers of each region, especially as regards the training of pharmacists. The sustainability of pharmacists as vaccinators will depend on their level of expertise and impact made, hence lots of emphasis should be placed on training. Strategies for improving the health literacy of populations in different regions should be considered.
Steering the conversation from ‘vaccination’ to ‘life-course immunisation’ in pharmacy
A good strategy will be to emphasize the economic benefits of establishing a life-course approach to immunisation. The ageing population, vaccine hesitancy, and high antimicrobial resistance levels add pressure to health systems. A life-course approach to immunisation instead of restricting it to just childhood vaccination has potential economic benefits. These include improved individual and population health, healthy ageing, reduced health costs, improved workforce productivity, and reduced antimicrobial resistance spread. Life-course immunisation could also support equity and universal access to primary care by providing a platform for the delivery of these services. Consequently, these will strengthen health systems, support health system sustainability, and promote economic prosperity. Emphasizing these benefits make life- course immunisation a critical priority and create that opportunity for its establishment. A good starting point will be to commence with vaccines that are widely accepted such as the influenza vaccine and then expand the range of vaccines and age range.
Trust is an important driver of vaccine acceptance. As pharmacists are widely renowned as the most accessible healthcare professionals, they should endeavour to build trust with the communities they serve concerning immunisation. Improved trust with the public will enhance acceptance of pharmacy-based vaccination services, thereby creating an avenue for pharmacists to improve health literacy, create awareness about the importance of life-course immunisation, and bolster pharmacists’ recognition as vaccinators. Hence, pharmacists need to be equipped with the requisite knowledge and skill to be extremely good communicators, competent in vaccinating all ages, and understand administration, and supply chain. This can be achieved by developing an immunisation course that will provide credentialing for pharmacists.
Pharmacists should advocate for policies that promote life-course vaccination as a means of promoting healthy ageing, improve the vaccination rate among healthcare professionals (including pharmacists), empower pharmacists as vaccinators, include pharmacies as vaccination sites, develop patient knowledge and improve attitudes and beliefs. Specific actions to actualize these goals should also be identified. For instance, new collaborations and private-sector partnerships to mobilize financing for vaccination of older groups could be established.
How FIP’s digital programme can support the identified priorities
Programmes should be developed that brings the entire FIP together for consultations, deliberations, and resolutions on transforming vaccination. These should encourage pharmacists to take up vaccination roles, empower them to proffer solutions to immunisation challenges, improve their confidence, enlighten them on their role in promoting health literacy, correcting misinformation and myths about vaccines. Video contributions that address vaccination across pharmacy education, workforce, and science from member organizations and individual members could be requested.
FIP’s work on vaccination is based on the assertion (and emerging evidence) that improving vaccination coverage and promoting a life-course approach to vaccination are global imperatives to which pharmacists can greatly contribute. With adequate training, pharmacists are competent to perform a series of roles that can significantly contribute to improving vaccination coverage, from providing evidence-based advice on vaccines and addressing vaccine hesitancy and complacency, to administering vaccines and managing vaccination records. Although pharmacists have administered vaccines in several countries for years, this role is still new or even unknown to the profession in many parts of the world.
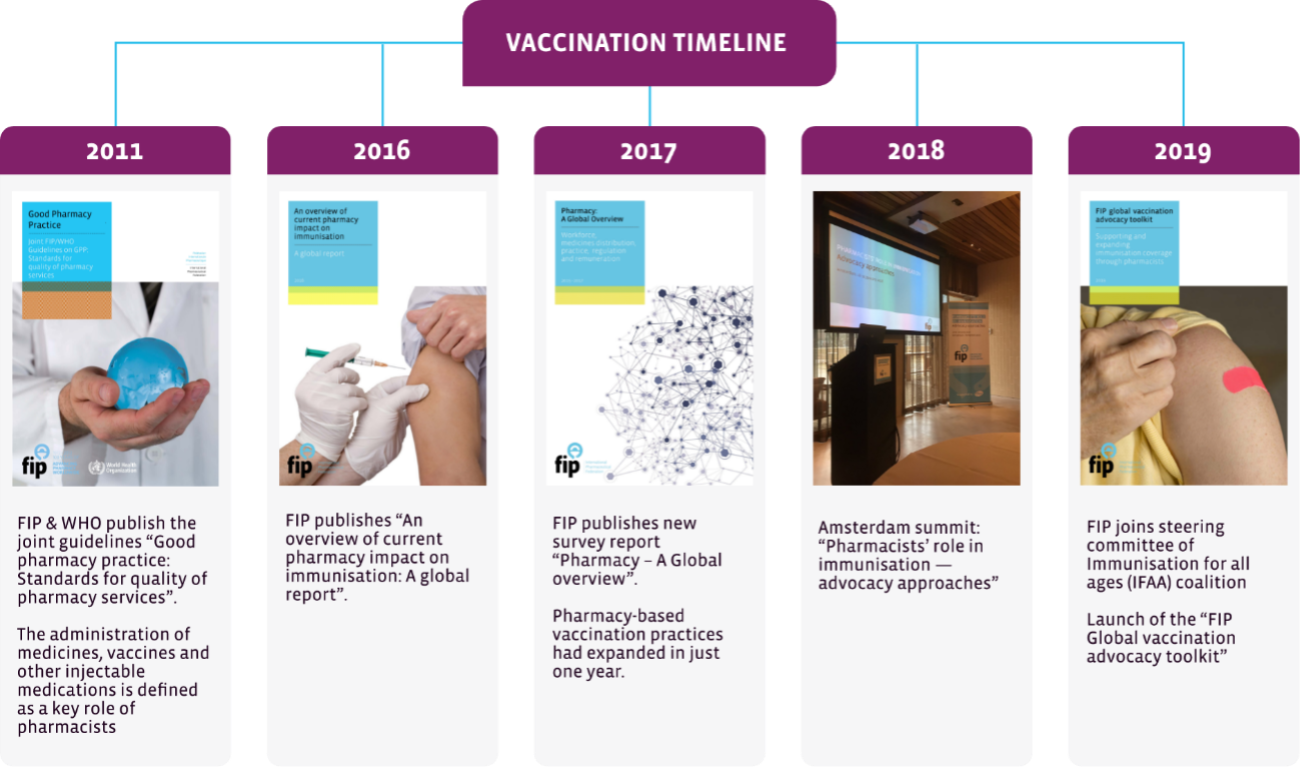
A recent timeline of FIP’s work on the area of vaccination can be found below in Figure 1.
Figure 1 - Timeline for FIP's work on vaccination


9.1 Recent publications
 9.1.1 FIP vaccination handbook for pharmacists: Procedures, safety aspects, common risk points and frequent questions - (2021)
9.1.1 FIP vaccination handbook for pharmacists: Procedures, safety aspects, common risk points and frequent questions - (2021)
This FIP handbook compiles the various roles that pharmacists play, that contribute towards improving vaccination coverage rates and access to vaccination services across all ages and population groups.
It supports individual pharmacists with understanding how they can contribute to improving vaccination coverage through a range of services, from patient education and advice, to logistical roles and to the administration of vaccines.
This FIP handbook provides guidance on the practical implementation of these services and includes guidelines on the procedures, safety aspects, common risk points and frequently asked questions about vaccines and their administration. The publication can be accessed here.
 9.1.2 Building vaccine confidence and communicating vaccine value - A toolkit for pharmacists - (2021)
9.1.2 Building vaccine confidence and communicating vaccine value - A toolkit for pharmacists - (2021)
This FIP toolkit describes specific roles that the pharmacy workforce play in addressing vaccine hesitancy and concerns. It supports individual pharmacists with tools for effectively communicating the value, efficacy and safety of vaccines, and for addressing concerns about or the rejection of vaccines.
It provides a background on vaccine hesitancy and the main reasons for it as well as ways to address vaccine hesitancy directly with individuals. It also includes examples of pharmacy-based campaigns and information, and guidance on advice for different types of vaccines. The toolkit can be found here.
9.1.3 Pharmacy based pandemic vaccination programme: regulatory self-assessment tool - (2021)
 This self-assessment tool helps to identify strengths and areas for improvement in order to inform pandemic planning efforts ahead of current and future waves of COVID-19. It is an aid to help national ministries of health and regulators in assessing pandemic preparedness and the state of legislation and regulations within their countries to facilitate mass vaccination and testing and enhanced patient care through pharmacists and community pharmacies.
This self-assessment tool helps to identify strengths and areas for improvement in order to inform pandemic planning efforts ahead of current and future waves of COVID-19. It is an aid to help national ministries of health and regulators in assessing pandemic preparedness and the state of legislation and regulations within their countries to facilitate mass vaccination and testing and enhanced patient care through pharmacists and community pharmacies.
This self-assessment tool seeks to help with vaccination planning and mitigate risk of future waves of COVID-19. While this tool is not exhaustive, and not yet validated, it is based on the experiences of professional regulators in countries where pharmacy-based vaccination and testing have been successfully introduced and regulated and, as such, seeks to be a supportive tool. Please find this publication here.
9.2 Recent digital events
9.2.1 Event series - “Joining forces towards improved vaccination access and coverage rates — High-level roundtables”
Vaccination coverage rates for several diseases are suboptimal and remain below WHO targets in many countries of all income levels. As such, FIP considers that it is essential to promote dialogue and increase understanding around these perceptions among healthcare professionals’ organisations at the international level, so that these can be cascaded to the regional, country and local levels.
This series of two high-level roundtables included an event with FIP’s sister organisations for the other healthcare professionals (the World Medical Association, the International Council of Nurses, the World Dental Federation – FDI, World Physiotherapy and FIP) and one with civil society organisations. The latter included representatives from different constituencies, including the International Federation on Ageing, the Active Citizenship Network, the International Diabetes Federation, the International Primary Care Respiratory Group, and Vaccines Today. The goal was to discuss and outline synergistic and complementary advocacy actions for broader access and convenience of vaccination services through a diversity of providers and pathways. Details from this series can be found below.
|
Joining forces across health professionals towards improved vaccination coverage 29 June 2021 |
 |
|
Joining forces across civil society organisations towards improved vaccination coverage 21 October 2021 |
 |
9.2.2 Event series - “Building vaccine confidence together”
The World Health Organization lists vaccine hesitancy—concerns related to vaccination or outright refusal to receive vaccines despite availability—as one of the top ten threats to global health in 2019. This threat is evidenced by recent outbreaks of vaccine preventable diseases in many high-income countries and the sheer volume of disinformation circulating regarding the recently approved vaccines against novel Sars-Cov-2 virus.
Often, “one-size-fits-all” vaccine promotion efforts can backfire when presented to individuals who are already sceptical of vaccines.
These events outlined evidence-based strategies for developing pharmacist-led interventions which focus on communication with patients in order to build vaccine confidence and improve uptake and in immunization campaigns which communicate the value of vaccines to specific patient groups in order to build vaccine confidence and improve uptake.
Details for this series can be found below.
|
Developing effective pharmacy-led vaccination campaigns 26 July 2021 |
 |
|
Understanding vaccine hesitancy and building vaccine confidence through effective conversations 8 September 2021 |
 |
9.2.3 Digital event - Increasing vaccination coverage through pharmacists
Although pharmacists have administered vaccines in several countries for years, this role is still new or even unknown to the profession in many parts of the world. As a role that involves direct contact with the patient and the administration of a product by injection, it may still generate some concerns among pharmacists with regards to the administration procedure, common errors and the management of anaphylactic reactions. This webinar described such procedures and addressed common questions and concerns. Details from this series can be found below.
|
Vaccine administration routes and procedures: frequent concerns and common errors 13 Jan 2021 |
 |
9.2.4 Digital event - Infodemic and vaccine hesitancy response
This digital event discussed how important it is to promote confidence in influenza vaccines and avoid complacency towards vaccination due to lower influenza rates in the past year. Harnessing the convenience of access to pharmacies will be paramount to achieve these goals.
Due to the widespread adoption of disease prevention measures to reduce transmission of COVID-19, the prevalence of the seasonal influenza lowered drastically around the world. However, as more people become vaccinated against COVID-19 and measures such as mask wearing, social distancing and home-based working or schooling are eased, the flu could return with high incidence rates and people could be more susceptible to the influenza virus due to lack of recent exposure. Developing flu vaccines in 2021 was also more challenging than usual due to less available data. This uncertainty around the return of influenza makes vaccination all the more critical, and it essential to communicate this to the population. Details from this series can be found below.
|
Confidence, complacency and convenience: Key elements of influenza vaccination strategies in times of COVID-19 12 Oct 2021 |
 |
9.2.5 Digital event - Presentation of the technical document “Pharmaceutical services in immunisation: contributions, experiences and implementation in the Americas region”
The document "Pharmaceutical services in immunisation: Contributions, experiences and implementation in the Americas region", authored by the Drug Information Centre of the Pharmaceutical Research Institute of the Faculty of Pharmacy of the University of Costa Rica for the Pharmaceutical Forum of the Americas, provides an overview of the involvement of the pharmacy profession in immunisation in Latin America. This introductory webinar will provide an overview of the document’s content and how it relates to the FIP Development Goals. This document is intended to be a tool for the implementation of pharmaceutical services in immunisation in the region, which also complements other reports issued by FIP. The document is available in Spanish, English and Portuguese. Details from this event can be found below.
|
Presentation of the technical document Pharmaceutical services in immunisation: contributions, experiences and implementation in the Americas region. 17 Nov 2021 |
 |
Series 1:
Jane Barratt, Daphne Holt, Lois Privor-Dumm, Carlene McMaugh, Nadia Bukhari, Sofia Segura, Samiratou Ouedraogo, Erica Rosser, Timothy Chen, Mujahidhussein Valji, Fiona Stanaway, Regis Vaillancourt, Hannelie Meyer, Eduardo Savio, Suresh Bhojraj, Meghna Joshi-von Heyden, Marleen Haems, and Katarina Milosevic Kostadinovic
Series 2:
Nuria Montero Chinchilla, Carlos Lacava, Eduardo Savio, Magaly Rodriguez, Sofia Segura, Kasey Thompson, Martha Rebour, César Moreno Romero, and Mariela Mendez Ferreira, Ayman Noreddin, Ziad Nassour, Madeeha Malik, Mohammed Al-Nuzili, Ahmed Abdulbary, Rula Darwish, Ema Paulino, Stephanie Kohl, Koen Straetmans, Piotr Merks, Vibhu Paudyal, Monika Derecque-Pois, Mary Ann Sant Fournier, Chinta Abayawardana, Sherly Meilianti, Vindya Pathiraja, Suresh Bhojraj, Keri Lestari, Rao Vadlamudi, Sanjeev Sharma Kattel, John Jackson, Parisa Aslani, Stephanie Tay, Leonila Ocampo, Chris Campbell, and Amrahi BuangProsper Hiag, Daniella Munene, Samuel Adekola, Redouane Soualmi, Mariet Eksteen.
FIP Leadership, members & partners:
FIP President Dominique Jordan; FIP Executive Committee & Bureau; FIP Members; FIP Partners; FIP YPG; and the Regional Pharmaceutical Forums & regional leaders.
FIP Transforming Vaccination Programme Project Team:

Thank you to FIP Staff, Gonçalo and Rúben, for their additional support through their contribution to the collection.
Events, Marketing and Communications Team:
Sponsor & supporter Pfizer:

